2022 Pediatric Respiratory Surge Event #7
Healthcare Ready is ENGAGED for this event. We are monitoring potential concerns for supply chain disruptions and impacts on healthcare services.
Highlights and Key Updates
- On 12/2, Secretary of the Department of Health and Human Services Xavier Becerra sent a letter to state governors providing guidance on how to deal with the pediatric hospitalization crisis. The letter reiterates the resources and tools that are available, including flexibilities under the COVID-19 PHE declaration, as well as nearly $400 million in funding from the Centers for Disease Control (CDC) slated for preparedness and response activities, including respiratory diseases. An example of the letter, the one sent to the Washington State’s Governor Jay Inslee, may be viewed on the Washington State Hospital Association’s (WSHA) website.
- As of 12/08, there is no response to AAP and CHA’s November 15 letter calling for government officials to declare a public health emergency for RSV. Federal officials point to the lack of local and state requests for an emergency declaration through departments of health and mayoral/gubernatorial offices.
- Healthcare Ready recommends healthcare systems advocate for local declarations to access immediate resources at the state and regional levels.
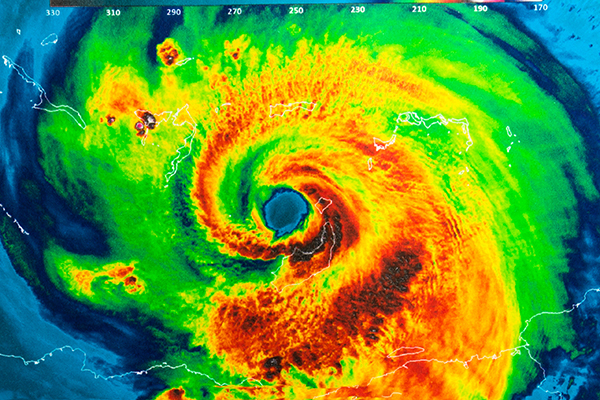
- Healthcare Ready is regularly updating a map showing HHS data on pediatric hospital bed utilization. The map was last updated with data from 12/6.
- Healthcare partners are reporting that many facilities’ pediatric bed capacity is compared to the number of licensed beds for a facility, instead of staffed and equipped beds. This may be artificially inflating bed availability in many places experiencing staffing and equipment shortages. Healthcare Ready is working to develop a new model for bed availability reporting but will report official data in the meantime. Our mapping tool notes this complication.
- As of 12/6, 72.6% of pediatric beds are occupied (-2.87 percentage points from 11/30), with five states reporting bed utilization above 90%.
- As of 12/06, states with the highest rates of in-patient pediatric bed utilization are: Idaho: 150.67% (+46.17 percentage points), Nevada; 97.29% (+0.66), Arizona: 93.97% (-4.34), Rhode Island: 93.56% (-0.13), Utah: 91.73% (-5.47), District of Colombia: 88.57% (+1.75). Oregon: 88.29% (-1.32), Minnesota: 88.00% (-0.54), Texas: 87.71% (+07.24), and Missouri: 81.98%.
- As of 11/08, Idaho state officials have not passed emergency measures concerning the pediatric surge crisis despite Idaho reporting hospitals functioning at over 150% of their pediatric bed capacity.
- If the COVID-19 PHE is not renewed before its expiration in mid-January 2023, between 5.3 and 14.2 million Medicaid enrollees could lose their coverage between January and April 2023.
- On 12/1, NMDOH issued a public health order facilitating inter-hospital communication, monitoring oxygen supply and any possible shortages, issuing waivers from the state’s department of health, and distributing public health advisories to New Mexico residents in English, Spanish and other languages.
- On 12/7, Oregon Governor Kate Brown issued executive order No. 22-24, expanding the 11/14 declaration and calling for Oregon Health Authority (OHA) and other state agencies to deploy volunteer emergency health care workers and designate emergency health centers.
- Several manufacturers report limited or no supply of certain oseltamivir formulations (an influenza antiviral).
- Multiple jurisdictions issued an advisory permitting compounding of oseltamivir suspension on a limited prescription basis. The advisories noted that practitioners may prescribe oseltamivir capsules and provide patient’s guardians with CDC guidance on opening and mixing capsules with liquids for children who might not be able to otherwise swallow it.
Assessment of Healthcare Logistics Impacts
Background
The confluence of RSV, influenza, and COVID-19 is creating a surge in severe pediatric respiratory illnesses and hospitalizations that threaten healthcare delivery systems. Influenza and RSV activity are higher than usual for the time of year, perhaps due to pandemic related preventative measures being relaxed. It is not yet clear how the surge in respiratory illnesses will impact the capacity of facilities, such as community health centers, free and charitable clinics, urgent care, or pharmacies. These facility types will be critical for case identification and first-line treatment.
Healthcare Ready is working to understand these impacts to best support communities with the greatest needs.
Pediatric Hospitalizations
- As of 12/6, 72.6% of pediatric beds are occupied (-2.87 percentage points from 11/30), with five states reporting bed capacity above 90%. Bed utilization estimates may be underestimated due to low participation from hospitals reporting into HHS TeleTracking. For 12/6 data, 67% of US hospitals were reporting. Local capacity may vary drastically within a given state as not all hospitals are reporting and/or some hospitals reporting may not. As such, hospital capacity is likely even more strained than reflected in this data.
- As of 12/06, states with the highest rates of in-patient pediatric bed utilization are: Idaho: 150.67% (+46.17 percentage points), Nevada; 97.29% (+0.66), Arizona: 93.97% (-4.34), Rhode Island: 93.56% (-0.13), Utah: 91.73% (-5.47), District of Colombia: 88.57% (+1.75). Oregon: 88.29% (-1.32), Minnesota: 88.00% (-0.54), Texas: 87.71% (+07.24), and Missouri: 81.98%.
- Healthcare Ready is regularly updating HHS data on pediatric hospital bed utilization (snapshot, below).

Confluence of RSV, COVID-19, and Influenza
- New hospitalizations for respiratory illnesses, especially influenza and COVID-19, are spiking following the Thanksgiving holiday. Flu hospitalizations “remain at a decade high” and COVID-19 hospitalizations have increased more than 20% compared to the previous week.
- While RSV may have peaked in some areas, overall increases in hospitalizations from COVID-19 and flu in adult and pediatric populations puts additional strain on hospitals that are already at or above capacity. Such strain, especially with months of the respiratory season still ahead, may further constrain capacity to care for critically ill patients of all ages across the US.
- Some facilities have reported upticks in illness in staff, creating staffing impacts that further constrain the surge capacity of hospitals and other facilities.
- CDC is encouraging use of masks to help prevent spread of COVID-19, flu, and RSV during the holiday season.
- The uptake of COVID-19 and influenza vaccines will be a crucial factor for limiting respiratory-related hospitalizations throughout the winter months.
- Vaccination rates of children for both COVID-19 and influenza remain very low. American Academy of Pediatrics analysis based on CDC data shows only 10% of children aged 6 months to 4 years old have received at least one dose of the COVID-19 vaccine.
- As of 11/19, about 40% of children between the ages of 6 months and 17 years have been vaccinated for influenza for the 2022-2023 season.
RSV
- Data shows that rates of RSV cases and hospitalizations may have peaked in some areas of the US. However, lack of comprehensive localized (smaller than state-level) data leaves gaps in national picture of when and where cases are peaking. Disclaimer: The following analysis is based on the limited available data for RSV.
- CDC National Respiratory and Enteric Virus Surveillance System (NREVSS) RSV laboratory test data show:
- RSV cases in HHS Region 8 (Montana, Wyoming, Utah, Colorado, North Dakota, and South Dakota) have not yet peaked. State level data shows a continuous upward trend in 3 week averages for RSV PCR test positivity in Montana and Wyoming. PCR test positivity for North Dakota and Colorado indicates cases in those states may have peaked or are currently peaking. South Dakota’s PCR test positivity has shown an inconsistent (not continuous) upward trend; it is unclear if this indicates a peak in cases. Data for Utah is not available.
- Cases in Region 10 (Washington, Oregon, Idaho, Alaska) may be peaking. State level 3 week averages for RSV PCR suggests cases in Washington state may have peaked, but are likely still rising in Idaho. Cases in Oregon and Alaska may be peaking currently.
- No update to RSV-NET data since last report. The data from CDC’s RSV-NET* for the week ending 11/26 shows a decrease of RSV-related hospitalization rates in most demographics, including children ages 6 months to 4 years. The non-representative dataset shows declines in hospitalizations across race and ethnicities and age groups (data accounts for about 8% of the US and actual trends may be higher).

- *RSV-NET data represents only the aggregated data from participating states (8% of the US). Hospitalizations may be higher due to the increased likelihood of non-laboratory confirmed RSV cases and lack of data for potentially vulnerable populations.
- Guidance for assessing and prioritizing bronchiolitis patient needs is available in resources such as East Tennessee’s Children’s Hospital’s Bronchiolitis Care Map and Spectrum Health’s Clinical Pathway: Pediatric Bronchiolitis, Inpatient.
- ASPR TRACIE released guidance on use of high flow nasal cannulas (HFNC) in pediatric patients, including the clinical pathways, decision support tools, and information on use of HFNC in non-intensive care unit settings and during patient transport.
Influenza
- Influenza-associated pediatric deaths rose to 14 (+5) for 2022-2023 flu season as of the week ending 11/26.
- Three of the 14 influenza-associated pediatric deaths were recorded in Alabama.
- The 2022-2023 influenza season is the most severe in terms of hospitalizations for the time of year in 13 years. According to CDC, “the cumulative hospitalization rate… is higher than the rate observed in week 47 during every previous season since 2010-2011.”
- Influenza-like illnesses (ILI) levels are very high across the United States. Forty-six states, New York City, Puerto Rico and the District of Columbia are experiencing high to very-high levels of ILI. Twelve of the jurisdictions are reporting ILI activity level 13, the highest possible. Those states are: California, Colorado, Kentucky, Nebraska, New Mexico, Ohio, South Carolina, Tennessee, Texas, Virginia, Washington, and New York City.
- The ILI activity level denotes the intensity of the ILI activity and not the geographic spread. Thus, an entire state might display as high due to a reporting entity reporting surge capacity to the point that the jurisdiction does not have the available resources to compensate.
- Very high ILI activity, levels 11-13, indicates that flu activity is 12-20 standard deviations present above the mean, indicating that the area’s infrastructure, workforce, and supply chain capacities might not be able to accommodate local needs without additional assistance.
- The test positivity rate rose by 6.88 percentage points between the week ending 11/19 (18.22%) and the week ending 11/26 (25.1%).
- For the week ending in 11/26, the 0-4 age group experienced the highest rates (17.5%) of outpatient visits for influenza-like illnesses.
- All age groups saw a percentage increase in positivity rates from the previous reported week with age 5-24 years experiencing the largest percentage point increase of 2.9.
- Aggregated data of all age groups demonstrates that the youngest populations are disproportionately contracting respiratory illnesses.

COVID-19
- The COVID-19 public health emergency (PHE) provides a variety of federal, state, and local flexibilities in regulation and funding support for the response to RSV and flu. If the COVID-19 PHE is not renewed before its expiration mid-January 2023, between 5.3 and 14.2 million Medicaid enrollees could lose their coverage between January and April 2023.
- Between February 2020 and August 2022, the Medicaid/Children’s Health Insurance Program (CHIP) enrollment rose by 27.1% or 19.3 million enrollees. At least 5.8 million of those enrollees were children, per reporting from states that report those statistics separately from the adult ones.
- If the existing PHE is not renewed or a pediatric surge PHE is not declared by the federal government, millions of children could lose access to healthcare coverage due to disenrollment in CHIP. This could lead to severe health impacts for those currently enrolled, on the individuals and underserved communities, The end of the PHE could have additional impacts on funding for federal and state government programs.
- Between February 2020 and August 2022, the Medicaid/Children’s Health Insurance Program (CHIP) enrollment rose by 27.1% or 19.3 million enrollees. At least 5.8 million of those enrollees were children, per reporting from states that report those statistics separately from the adult ones.
- National-level data continues to shows an increase in new hospital admissions of pediatric patients with confirmed COVID-19 compared to the prior week. New admissions of elderly patients also increased since the week ending in 11/26. New admissions of patients with confirmed COVID-19 have shown a continuous upward trend that began in late October. As of 12/07, compared to the average admissions for the week ending 11/26:
- People ages 0-17: +20.7% new admissions per 100,000
- People ages 70+: +16.5% new admissions per 100,000
- Federal funding for COVID-19 vaccines might run out as early as in January 2023, at which point COVID-19 vaccines and therapeutics will become available only via the commercial market.
- According to an analysis from the Kaiser Family Foundation, “private insurers will be required to take on more of the cost of vaccines (including paying for the doses themselves once the federal supply runs out), which could have a small upward effect on premiums.”
- Implications for how these changes may affect vaccine availability and out-of-pocket costs to patients will become clearer as the commercial cost of vaccines and mechanisms for distribution and purchasing are defined.
- A new study published on 12/1 analyzing severe COVID-19 outcomes in pediatrics found that Omicron variants had the highest hospital admission rates while Alpha and Delta variants caused more severe illness (defined as a composite of intensive care unit admission, mechanical ventilation use, and conditions such as viral coinfection, myocarditis, and death). Alpha and Delta variants caused higher instances of Multisystem Inflammatory Syndrome in Children than Omicron. Viral coinfection was more common with Delta and Omicron variants, while to a lesser degree. The study also finds that the “coinfection with respiratory viruses increased the risk of severe outcomes and impacted infants more than older children.”
- If the upward trend of COVID-19 hospitalizations continues into the respiratory season, healthcare institutions might end up dealing with compounded crisis conditions and surge, putting further strain on healthcare infrastructure and workforce of these multiple populations.
Health Equity Concerns
- Some reporting suggests pediatric patient transport, which is already constrained due to staffing, availability of hospital beds that are staffed to receive a patient, and specific supplies needed to transport a child, is especially challenging for rural areas. Ability for rural areas to move patients, especially across state lines, may be limited.
- Children with underlying conditions, especially obesity and diabetes, are more likely to experience severe COVID-19 and hospitalization. According to data from CDC’s COVID-19 Associated Hospitalization Surveillance Network (COVID-NET), during the 2021-2022 Omicron surge (December 2021 – February 2022): 70% of hospitalized children had an underlying medical condition, 19% were admitted to an intensive care unit, and children with diabetes and obesity were more likely to experience severe COVID-19.
- For the limited areas tracked by CDC’s RSV-NET* for the week ending 11/26, hospitalization rates for all races and ethnicities have fallen compared to the previous week.

- Infants younger than six months, especially those born premature, are at an especially high risk of contracting RSV. Other populations vulnerable to worse impacts to RSV, including higher hospitalization rates, include black children, pregnant people, older adults, older adults with comorbidities, the uninsured, and those living below the poverty line. A study published in 2021 found that those living in census tracts with higher rates of poverty were more likely to be hospitalized with RSV.
- Past research shows that patients of color and those from low-income or limited English proficiency families are more likely to experience worse hospital outcomes compared to other children. The same socio-economic factors increase the likelihood for hospitalization due to RSV. Clinicians should be aware of the potential of implicit bias due to structural racism to impact treatment of pediatric patients of color and interactions with their families. Systemic racism not only impacts the quality of care that people of color receive, but also reduces their likelihood to seek care for fear of mistreatment.
- A study found that multi-generational households and general “crowding” in the household were associated with an increased rate of RSV in high-risk children under the age of five.
- Alaska Natives (AN) have historically been a particularly vulnerable group to RSV. In general, AN children experience one of the highest rates of hospitalization for lower respiratory tract infections and RSV among children in the US.
- Healthcare Ready centers building equity into preparedness, response, and recovery resources, including this report. To learn more about Healthcare Ready’s core belief of why it is important to highlight vulnerable populations during disasters, read our Equity Framework.
Government Response
Federal Posture
- On 12/2, Secretary of the Department of Health and Human Services Xavier Becerra sent a letter to state governors providing guidance on how to deal with the pediatric hospitalization crisis. The letter reiterates the resources and tools that are available, including flexibilities under the COVID-19 PHE declaration, as well as nearly $400 million in funding from the Centers for Disease Control (CDC) slated for preparedness and response activities, including respiratory diseases. An example of the letter, the one sent to the Washington State’s Governor Jay Inslee, may be viewed on the Washington State Hospital Association’s (WSHA) website.
- CDC Director Rochelle Walensky, in a respiratory disease update call with reporters on 12/5, encouraged people to mask to help prevent the spread of influenza, RSV and COVID-19 over the holiday season as the influenza-associated hospitalizations nearly doubled the week of Thanksgiving (19,593) compared to the prior week 46 (11,378) and are almost 40 times higher than the same week (495) last year.
- On 12/1, Surgeon General Vivek Murthy spoke about implementing measures to mitigate the pediatric surge, how to prepare for winter months, and how the federal government is working with healthcare institutions and workers across the nation. Murthy urged COVID-19 and flu vaccinations for parents and children, and to speak with their provider about getting Paxlovid if they start experiencing symptoms.
- There is currently no declared federal public health emergency (PHE) for pediatric surge.
- An emergency declaration would grant waivers for certain Medicare and Medicaid programs and the Children’s Health Insurance Program (CHIP).
- PHE waivers for Section 1135 of the Social Security Act waiver would allow for easier movement or transfer of patients, use of new spaces for care, creation of offsite triage to manage capacity challenges, adaptation to workforce shortages, and licensure reciprocity to enable cross-state care, including telehealth.
- CDC issued an official Health Advisory on 11/14 about rising rates of RSV and the co-circulation with COVID-19 and influenza and its potential impact on healthcare systems.
- HHS ASPR and TRACIE Pediatric Surge Resources page.
State and Local Posture
- California
- On 11/11, California Health and Human Services Agency issued a Guidance for Response to Surge in Respiratory Viruses among Pediatric Patients. The guidance prescribes space waivers and program flexibilities under Title 22 California Code of Regulations.
- On 10/31, Orange County, California, issued a Declaration of Health Emergency in Orange County.
- Colorado
- On 11/11, Governor Polis in Colorado signed an executive order amending and extending the current COVID-19 disaster declaration to include RSV, influenza, and other respiratory illnesses.
- Idaho
- As of 11/08, Idaho state official have not passed any declaration concerning the pediatric surge crisis despite some hospitals reporting being at more than 150% of pediatric bed utilization.
- Treasure Valley area of Southwest Idaho, which includes the state capital Boise, is dealing with a staffing shortage and its hospitals are not able to accommodate the influx of pediatric patients and area’s fast-growing population. In order to mitigate the situation, health facilities reported transferring patients out of state.
- Eastern Idaho Regional Medical Center in Pocatello, Southeast Idaho, has 2.5 times the pediatric patients than beds and has resorted to treating pediatric patients in adult units.
- Idaho’s Department of Health and Wellness regularly updates its Infectious Diseases website where it is tracking state flu and RSV activity.
- As of 11/08, Idaho state official have not passed any declaration concerning the pediatric surge crisis despite some hospitals reporting being at more than 150% of pediatric bed utilization.
- Illinois
- On 12/1, Illinois Department of Public Health (IDPH) issued an advisory that compounding of oseltamivir suspension on a limited prescription basis is permitted, and that physicians should consider adding “please compound if necessary” to their oseltamivir prescriptions. The advisory mentions that brand name Tamiflu (oseltamivir) package includes “Emergency compounding of an Oral Suspension from 75mg Tamiflu capsules (Final Concentration 6mg/mL) that may be used to dilute any 75mg oseltamivir oral capsule; the advisory reminds prescribers that they may prescribe oseltamivir capsules and provide patient’s guardians with CDC guidance on opening and mixing capsules with liquids for children who might not be able to otherwise swallow it.
- Maryland
- On 11/24, Maryland Department of Health (MDH) launched a state RSV dashboard.
- On 10/28, Governor Hogan in Maryland announced that hospitals will receive $25 million to aid in pediatric intensive care unit recruitment and staffing.
- Massachusetts
- On 11/21, Massachusetts Governor Baker extended a COVID-19 related policy allowing acute care hospitals to use alternative spaces to help facilities manage pediatric medical surge associated with RSV.
- Michigan
- On 11/23, a Spokesperson for the Michigan Health Department advised Michigan families to take steps to prevent the spread of respiratory illnesses after Michigan state health regulators received emergency appeals from two hospitals to expand hospital bed capacity.
- New Mexico
- On 12/1, New Mexico Department of Health (NMDOH) issued a public health order facilitating inter-hospital communication, issuance of waivers from the state’s department of health, monitor oxygen supply and any possible shortages and issue public health advisories to New Mexico residents in English, Spanish and other languages.
- On 12/5, NMDOH issued a press release on the 12/1 public health order reiterating that the order requires New Mexico hospitals to reactivate and take part in “hub and spoke” modality through which they will arrange transfers of patients and manage resources to ensure appropriate levels of care.
- Nevada
- On 12/5, Governor Steve Sisolak’s Office said that arrangements have been made to ensure pediatric hospitalization surge staffing needs are met by Nevada State Board of Nursing (NSBN) fast-tracking the licensing applications.
- New York
- On 12/2, New York Senator and Majority Senate Leader Charles E. Schumer spoke at a news conference at Wyoming County Community Center in western New York. The region is grappling with pediatric surge, especially Oishei Children’s Hospital in Buffalo. Schumer reiterated his previous stance and expanded the call for HHS to set temporary structures like screening tents, bolstering use of telehealth, moving patients across state lines, credentialling out-of-state providers and coordinating medical supply chains.
- Ohio
- On 11/9, the State of Ohio Board of Pharmacy issued guidance allowing pharmacies to compound amoxicillin by combining it with other drugs or via dilution.
- Oklahoma
- On 11/12, the Oklahoma State Department of Health allowed hospitals to designate adult beds for pediatric use.
- Oregon
- On 12/7, Governor Kate Brown issued executive order No. 22-24 expanding the 11/14 declaration of emergency and calling for Oregon Health Authority (OHA) and other state agencies to deploy emergency volunteer health care workers and designate emergency health centers.
- OHA is seeking up to $25 million of nurse staffing contracts to meet workforce demand related to the surge.
- On 11/22, two Oregon hospitals declared crisis standards of care, primarily to increase available staff.
- On 11/14, Governor Kate Brown issued an executive order No. 22-23 under ORS Chapter 401 to support hospitals during the pediatric RSV response, and Oregon declared a public health emergency.
- On 12/7, Governor Kate Brown issued executive order No. 22-24 expanding the 11/14 declaration of emergency and calling for Oregon Health Authority (OHA) and other state agencies to deploy emergency volunteer health care workers and designate emergency health centers.
Potential Threats for Pediatric Medical Surge
Several challenges are unique to managing pediatric medical surges, particularly for the healthcare workforce and supply chain. For one, pediatric hospitals require more intensive nursing resources to treat and monitor patients, especially in intensive care and neonatal intensive care units.
Additionally, pediatric supply chains can also be more vulnerable to supply chain disruptions, as some critical products have only one supplier or manufacturer capable of producing the necessary pediatric-specific equipment and supplies.
Product Availability
- Amoxicillin remains in short supply.
- As of 12/8, multiple forms of amoxicillin remain on the FDA and ASHP drug shortage lists. This includes tablets, capsules, and powder for suspension. Providers and patients continue to experience impacts.
- The American Academy of Pediatrics recently reported on alternative therapies during the shortage. Those therapies are amoxicillin tablets, capsules, or chew tabs for children. The formulations available are 500 mg tablets, 250 mg capsules, and 250 mg chew tabs.
- Tablets can be split/crushed to mix with any liquid or semisolid, like applesauce. This can be given orally or by tube. Capsules can be opened and mixed with any liquid or semisolid, like applesauce. This can be given orally or by tube. And lastly, chew tabs can be split.
- Amoxicillin remains on allocation to protect supply until more product is available.
- Tamiflu (oseltamivir), the nation’s most popular influenza prescription drug, remains in high demand. As of 11/29, both the oral suspension and capsule formulations of oseltamivir remain on the ASHP shortages list. Oseltamivir is not currently on the FDA shortage list.
- Other alternative influenza antivirals include Xofluza, Rimantadine, Zanamivir.
- Updated as of 12/5: FDA’s list of available antiviral medications for the 2022-2023 influenza season.
- FDA notes that while certain variations of Tamiflu are unavailable, there are a no current shortages (as of 12/7) among many of other companies.
- There are no current shortages for Relenza, Rapivab, and Xofluza.
- ASHP’s current drug shortages list includes the following drugs that could negatively impact treatment of RSV and other respiratory illnesses:
- As of 12/2: Oseltamivir Oral Suspension and Capsules of various sizes from 10 different companies have been added. While no reasons for the shortage was provided by the companies themselves, we can assume it was due to the increase in demand from the recent surge in respiratory illnesses. It is important to note that some formulations of the product are listed as “available.” The sizes/formulations that are in shortage will either release in late December 2022, are on allocation right now, or the company cannot estimate a release date.
- As of 12/6: 0.9% sodium chloride vials of various sizes from Fresenius Kabi and Pfizer have been added. The shortage is likely caused by increased demand, related to the application of sodium chloride for respiratory therapy. Pfizer has 0.9% sodium chloride 10 mL vials on backorder and the company estimates a release date of May 2023. Fresenius Kabi has 0.9% sodium chloride 10 and 20 mL vials on backorder and the company estimates a release date of mid- to late-December 2022.
- As of 12/6: 23.4% Sodium chloride injection of various formulations from Fresenius Kabi and Pfizer have been added. Both Fresenius Kabi and Pfizer have said the shortage is due to an increase in demand. Expected resupply dates are from mid-December 2022 to January 2023.
- As of 11/28: Ceftazidime Injection (and its generic name Tazicef) from Pfizer, Sagent, and BBraun have been added. The shortage is due to increased demand, likely due to the fact that ceftazidime is used to treat a wide variety of bacterial infections and providers could be prescribing this drug as a remedy to respiratory symptoms.
- As of 11/29: Rocuronium injection, used during tracheal intubation, is in shortage from several manufacturers due to increased demand and manufacturing delays. Estimated resupply dates vary based on manufacturer.
- FDA’s drug shortage database lists the following updates regarding drugs that may be related to treating respiratory illness:
- Reverified on 12/2: Amoxicillin oral powder for suspension is available for current customers from Hikma pharmaceuticals. As of 12/6 most of the amoxicillin oral powder product for suspension from Sandoz is unavailable while some has limited availability. Additionally, as of 12/6, products from Aurobindo and Teva are on allocation.
- Reverified on 12/6: albuterol sulfate, a bronchodilator for oral inhalation, manufactured by Akorn Pharmaceuticals, remains unavailable and is estimated to be back in stock by Q2 2023. A 5 mL version from Nephron Pharmaceuticals is available.
- Definitions for product shortage vary by organization. Healthcare Ready sources data from multiple organizations that maintain drug shortage lists, including:
- American Society of Health-System Pharmacists (ASHP), which defines a drug shortage as “a supply issue that affects how the pharmacy prepares or dispenses a drug product or influences patient care when prescribers must use an alternative agent.”
- US Food and Drug Administration (FDA), which defines a drug shortage as “a situation where the total supply of all versions of the approved product available at the user level will not meet the current demand, and a registered alternative manufacturer will not meet the current and/or projected demands for the potentially medically necessary use(s) at the user level.”
- On 11/22, the FDA issued an emergency use authorization (EUA) for the Lucira COVID-19 and influenza multiplex test for use in a point-of-care (POC) setting. This will expand the testing kit pool as well as reduce the strain on the testing kit supply chain as two tests are combined into one.
Treatments for RSV
A monoclonal antibody therapy called palivizumab is available as a precautionary measure to prevent severe RSV illness in certain infants and children at high risk for severe disease during the normal respiratory season. It cannot cure or treat children who are already suffering from severe cases of RSV; it is a preventative treatment.
- On 11/17, AAP updated its guidance: Given the known efficacy of palivizumab along with the unpredictable surge capability of RSV, AAP recommends programmatic consideration of providing more than five consecutive doses of palivizumab depending on the duration of the current RSV surge in a particular region of the country.
- Palivizumab is sold under the brand name Synagis, and is marketed by Sobi in the United States. Sobi purchased US rights to Synagis from AstraZeneca in 2018. Before COVID-19, physicians prescribed Palivizumab more frequently as a preventative measure, yet, this treatment strategy slowed during the pandemic.
- AAP says that it recommends Palivizumab in eligible infants in regions that are experiencing high rates of RSV and that it will release updated guidance as they monitor the seasonal trends.
Workforce Shortages
Workforce shortages continue to impact access to care in hospitals around the country. Resident physicians, doctors, hospitals staff are advocating for increased federal support.
Ongoing workforce shortages may threaten the ability for facilities to establish a predictable quality of care for patients. Because pediatrics is a specialty practice, there may be additional strain on the workforce with pediatric care experience. Reports indicate that pediatricians are requesting increased federal support as they deal with RSV, COVID-19, and influenza treatment in unison. Physicians state that they can only successfully handle this “tripledemic” with the assistance of a federal emergency declaration and dissemination of support.
Hospitals and other healthcare facilities may need to increase surveillance for respiratory illnesses among staff to reduce spread and the potential for staff being out sick. Practitioner mental health should also be considered and protected. Additional training and support for practitioners that are not used to caring for acute pediatrics cases for prolonged periods should be provided whenever possible.
About Healthcare Ready
Healthcare Ready is a 501(c)(3) nonprofit organization that works to ensure patient access to healthcare in times of disaster, emergency, and disease outbreaks. We leverage unique relationships with government, nonprofit and medical supply chains to build and enhance the resiliency of communities before, during and after disasters. Learn more about Healthcare Ready
To request the help of our Emergency Operations Center, contact us at alerts@healthcareready.org.
Sign up here.to receive email notifications from Healthcare Ready